2026

Moritz

Jakob

Maximilia

Mika

Azra

Magdalena

Diar

Nelio

Julian

Matti Elia


Liam


Liana Joy

Miriam

Maria Paulina

Paula


Thilo



Henry

Fritzi Juhl


Felix

Mila Valeria































































Bei der Kultivierung befruchteter Eizellen sind in den letzten Jahren deutliche Fortschritte erzielt worden. Soweit möglich versuchen wir mehrere befruchtete Eizellen weiter zu kultivieren und den Embryotransfer erst am Tag 5 nach Eizellentnahme im Blastozystenstadium vorzunehmen. Bei der Entwicklung bis zum Blastozystenstadium kommt es bei ca. 60% der befruchteten Eizellen zu einem Entwicklungsstopp. Diese natürliche Selektion während der Kultur führt dazu, dass oftmals nur 1 bis 2 wirklich gut entwickelte Embryonen das Blastozystenstadium erreichen.
Unser Ziel ist der single-embryo-transfer, also der Transfer eines gut entwicklungsfähigen Embryos, um möglichst eine Einlingsschwangerschaft zu erzielen. Überzählige Embryonen können ebenfalls kryokonserviert werden.
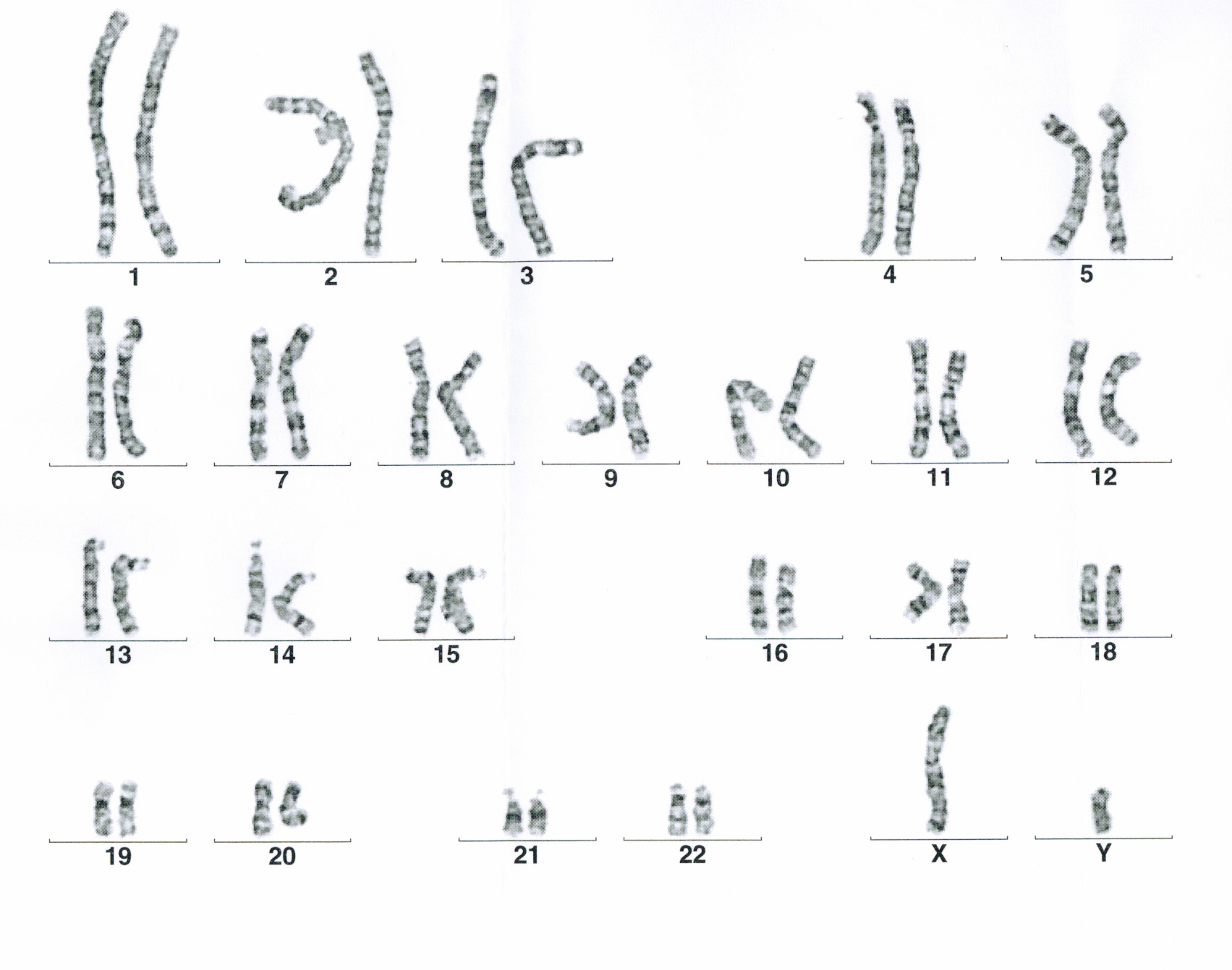
Vor Beginn der Therapie muss geklärt werden, ob eine konventionelle IVF oder eine ICSI notwendig ist. Der entsprechende Antrag auf Kostenübernahme kann bei Ihrer Krankenkasse gestellt werden. Diesen Antrag erhalten Sie von uns, nachdem wir Ihnen in einem Beratungsgespräch die Kosten- und Versicherungssituation erläutert haben. Für die ICSI-Therapie sind zwei Spermiogramme im Abstand von 12 Wochen erforderlich, die den Kriterien der Krankenkassen entsprechen. Es kann daher sein, dass nach dem Erstgespräch ein weiteres Spermiogramm erforderlich ist. Zusätzlich wird eine Chromosomenanalyse bei beiden Partnern empfohlen. In den neuen Richtlinien zur künstlichen Befruchtung 2017 ist festgelegt, dass Männer vor einer ICSI-Therapie von einem andrologisch qualifizierten Arzt untersucht werden müssen.

Sie müssen den Inhalt von reCAPTCHA laden, um das Formular abzuschicken. Bitte beachten Sie, dass dabei Daten mit Drittanbietern ausgetauscht werden.
Mehr InformationenSie sehen gerade einen Platzhalterinhalt von Turnstile. Um auf den eigentlichen Inhalt zuzugreifen, klicken Sie auf die Schaltfläche unten. Bitte beachten Sie, dass dabei Daten an Drittanbieter weitergegeben werden.
Mehr InformationenSie müssen den Inhalt von reCAPTCHA laden, um das Formular abzuschicken. Bitte beachten Sie, dass dabei Daten mit Drittanbietern ausgetauscht werden.
Mehr InformationenSie sehen gerade einen Platzhalterinhalt von Facebook. Um auf den eigentlichen Inhalt zuzugreifen, klicken Sie auf die Schaltfläche unten. Bitte beachten Sie, dass dabei Daten an Drittanbieter weitergegeben werden.
Mehr InformationenSie sehen gerade einen Platzhalterinhalt von Instagram. Um auf den eigentlichen Inhalt zuzugreifen, klicken Sie auf die Schaltfläche unten. Bitte beachten Sie, dass dabei Daten an Drittanbieter weitergegeben werden.
Mehr InformationenSie sehen gerade einen Platzhalterinhalt von Google Maps. Um auf den eigentlichen Inhalt zuzugreifen, klicken Sie auf die Schaltfläche unten. Bitte beachten Sie, dass dabei Daten an Drittanbieter weitergegeben werden.
Mehr InformationenSie sehen gerade einen Platzhalterinhalt von X. Um auf den eigentlichen Inhalt zuzugreifen, klicken Sie auf die Schaltfläche unten. Bitte beachten Sie, dass dabei Daten an Drittanbieter weitergegeben werden.
Mehr Informationen